Flap design: New perspectives in periapical surgery
September 28, 2017 / Categories: Digital Dentistry, Implant Dentistry

Peñarrocha Diago, Maria

Cervera Ballester, Juan
,
Abstract
Flap design in periapical surgery should be adequate for the planned surgical procedure, offering good access to the zone surrounding the affected apexes without altering the soft-tissue circulation.
A fullthickness flap including mucosa, submucosal connective tissue and periosteum should be raised. A description is provided of the most frequently used types of flaps in periapical surgery:
1. Luebke–Ochsenbein flap, involving submarginal incision, with semilunar or Partsch flap variants;
2. Neumann flap with intrasulcular incision in its triangular and trapezoidal versions;
3. papilla base incision flap;
4. papilla-preserving flap; and
5. palatal flap.
Designing the flap is a key aspect of periapical surgery: It should ensure adequate exposure of the surgical field and allow the surgeon to work quickly and comfortably. Furthermore, there should be no tension capable of complicating the work of the dental professional or of causing patient discomfort, and soft-tissue damage due to retractor compression is to be avoided. A good flap design with delicate manipulation of the soft tissue is necessary for successful periapical surgery.
Keywords
Periapical surgery, endodontic surgery, surgical technique, flap design.
Introduction
Two factors are important for securing optimum functional and esthetic outcomes in periapical surgery: flap design and the suturing technique used. Flap design in periapical surgery should be adequate for the planned surgical procedure, offering good access to the zone surrounding the affected apexes without altering the circulation in either the mobilized or nonmobilized soft tissue.1Arens DE. Flap design.
→ In: Arens DE, editor. Practical lessons in endodontic surgery. Chicago: Quintessence; 1998. p. 51–64.
A number of factors must be taken into account in preparing the flap: the location and extent of the apical lesion, the periodontal condition of the affected tooth and of the adjacent teeth, the condition of the surrounding anatomical structures, and the presence and quality of prosthetic restorations in contact with the gingival margin.2Arens DE. Flap design.
→ In: Arens DE, editor. Practical lessons in endodontic surgery. Chicago: Quintessence; 1998. p. 51–64. The flap should encompass at least one tooth on either side of the affected tooth. Acute flap angles are to be avoided. A narrow corner is difficult to trim and suture and can suffer ischemia and become detached, favoring the formation of scars.
A full-thickness flap including mucosa, submucosal connective tissue and periosteum should be raised. The interdental papilla should not be divided (sectioned) and should be either totally included within or separate from the flap. The incisions are to be sufficiently extensive to ensure that the retractor rests on bone and does not compress part of the flap.
Types of flaps
Classically, the most commonly used type of flap in periapical surgery has been the trapezoidal or triangular Neumann flap, with an intrasulcular incision and two vertical releasing incisions. However, owing to the improvements in surgical techniques and suture materials, oral surgery has become more conservative and delicate, and the Luebke–Ochsenbein flap with submarginal incisions is now more widely used.
Submarginal incision flap (Luebke – Ochsenbein flap)
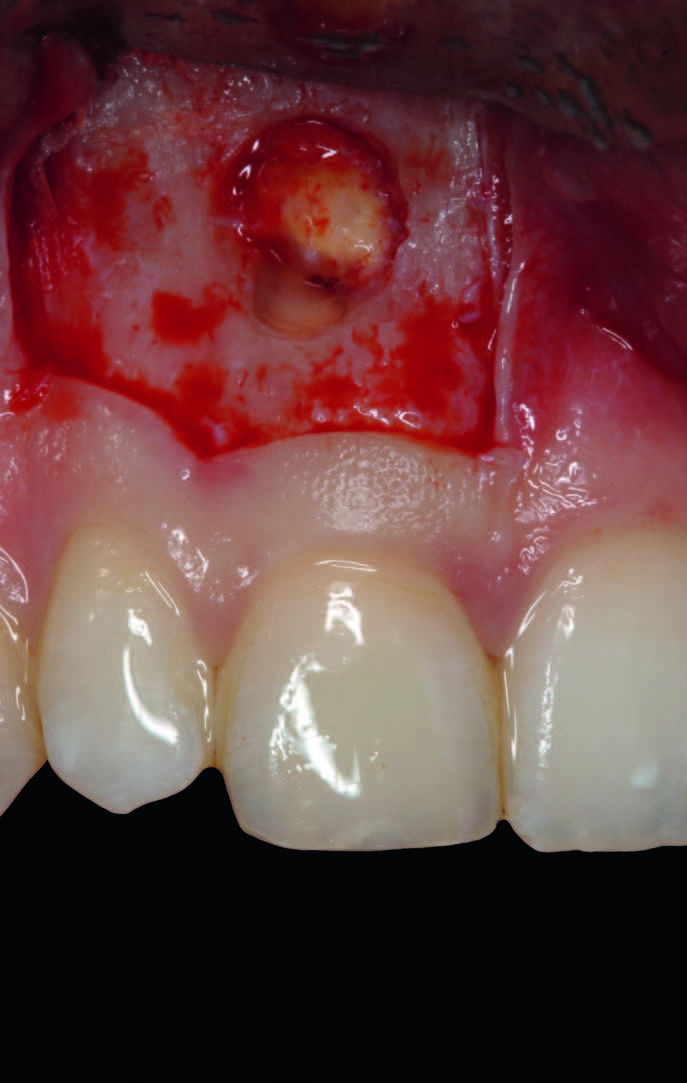
A horizontal incision is made in the attached gingival tissue about 3–4 mm above the gingival margin, with two vertical releasing incisions on either side of the flap located one or two teeth distal to where the lesion is located (Figs. 1–3). This type of flap is easy to detach, but can leave a postsurgical scar if the repositioning sutures are not performed adequately.3Vreeland DL, Tidwell E. Flap design for surgical endodontics.
→ Oral Surg Oral Med Oral Pathol. 1982 Oct;54(4):461–5.
-

-
Fig. 1
Clinical view before the trapezoidal submarginal flap for periapical surgery of tooth #11.

-

-
Fig. 2
Detachment of the trapezoidal submarginal flap.

-

-
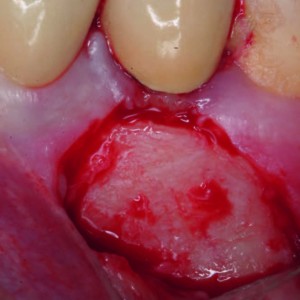
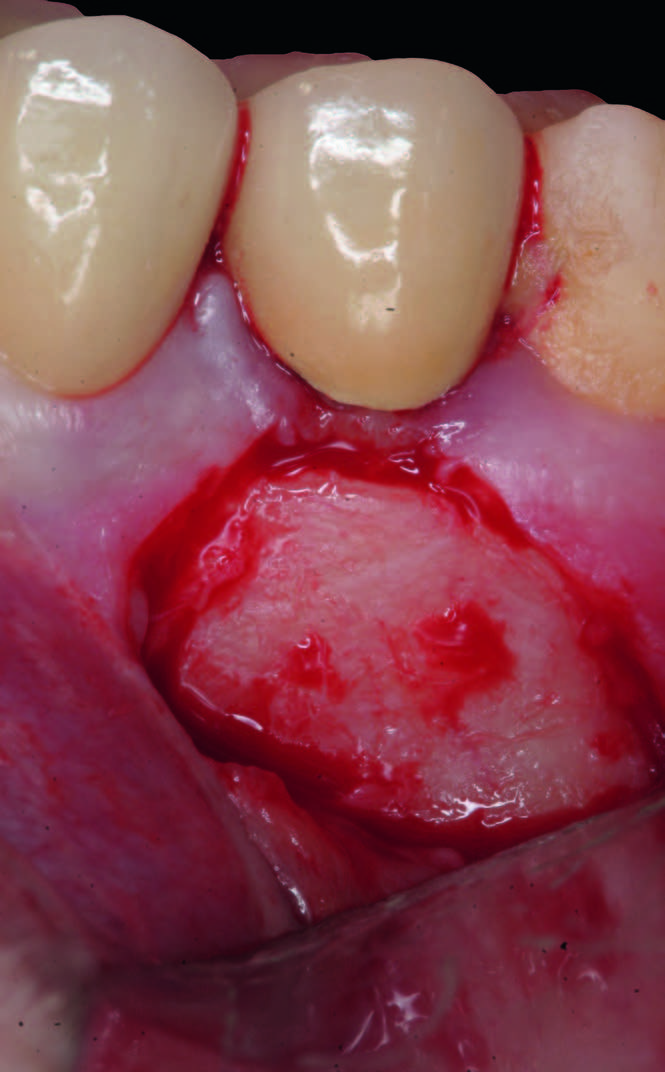
Fig. 3
Intraoperative view after ostectomy and resection of the apex of tooth #11.
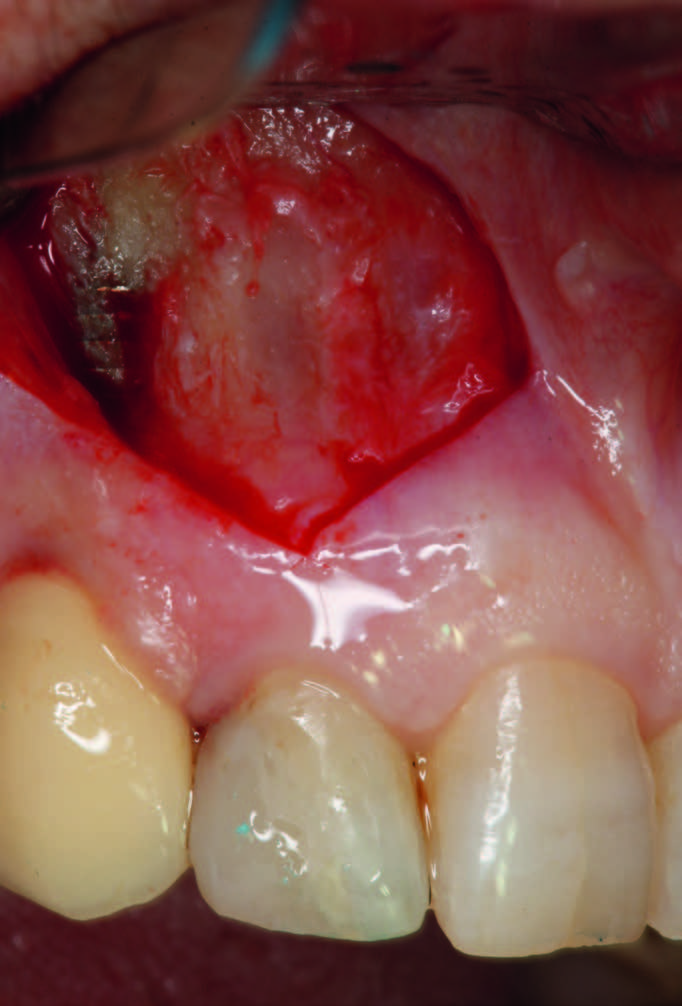
The Luebke–Ochsenbein flap is less aggressive with the gingival tissue than an intrasulcular incision flap, and it is easy to make the incision slightly triangular or angled in order to secure precise repositioning (Figs. 4–6). It is particularly useful in patients with fixed prosthesis restorations, since correct application of the technique results in less recession of the gingival margin 4Von Arx T, Vinzens-Majaniemi T, Bürgin W, Jensen SS. Changes of periodontal parameters following apical surgery: a prospective clinical study of three incision techniques.
→ Int Endod J. 2007 Dec;40(12):959–69.5Kreisler M, Gockel R, Schmidt I, Kühl S, d’Hoedt B. Clinical evaluation of a modified marginal sulcular incision technique in endodontic surgery.
→ Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009 Dec;108(6):e22–8. doi:10.1016/j. tripleo.2009.08.005. and interdental papillae.6Von Arx T, Salvi GE, Janner S, Jensen SS. Gingival recession following apical surgery in the esthetic zone: a clinical study with 70 cases.
→ Eur J Esthet Dent. 2009 Spring;4(1):28–45.
-

-
Fig. 4
Initial view before preparation of the triangular submarginal flap for periapical surgery of tooth #12.

-

-
Fig. 5
Detachment of the triangular submarginal flap.
-

-
Fig. 6
Clinical view showing the ostectomy for accessing the apex of tooth #12.
The semilunar (Partsch) flap is a variant involving submarginal incision in the alveolar mucosa to form a crescent- or semilunar-shaped flap. It is little used in periapical surgery because it affords limited surgical access to the root apex. Furthermore, owing to the presence of muscle fibers, flap tension is high, making suturing difficult and increasing the risk of suture dehiscence. 7Velvart P, Peters CI. Soft tissue management in endodontic surgery.
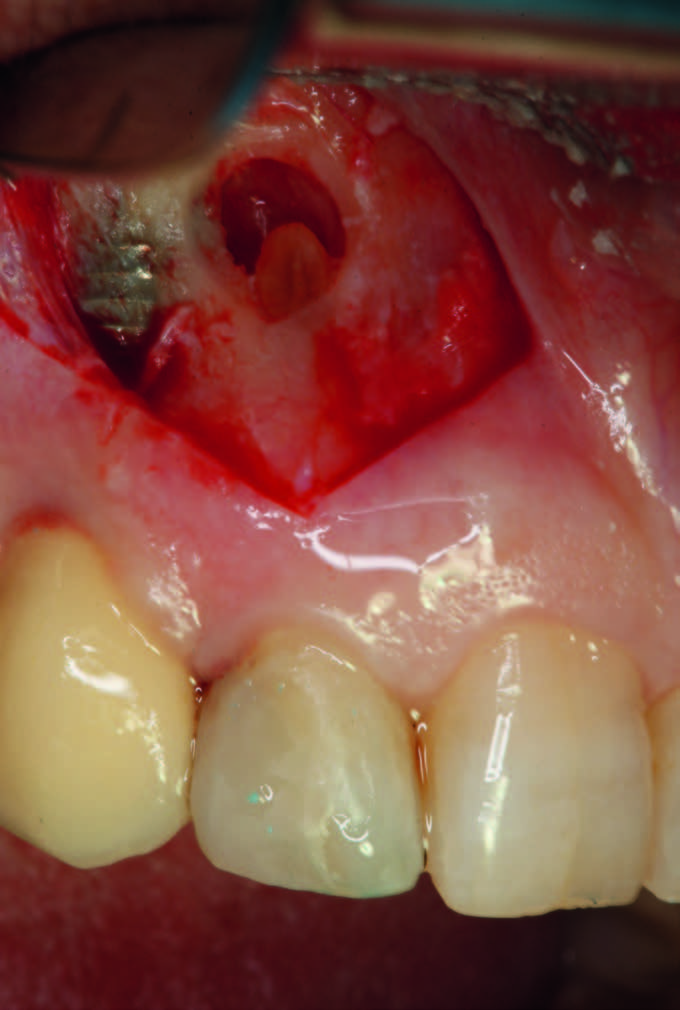
→ J Endod. 2005 Jan;31(1):4–16. The semilunar flap is almost exclusively used in application to the maxillary canines (Figs. 7–9).8Peñarrocha M. Técnica quirúrgica.
→ In: Peñarrocha M, editor. Cirugía periapical. Barcelona: Ars Medica; 2004. p. 45–79. Care is required to avoid performing the incision above the bone defect.
-

-
Fig. 7
Clinical view of tooth #23 before surgery.

-

-
Fig. 8
Detachment of the semilunar (Partsch) flap.

-

-
Fig. 9
Intraoperative view after ostectomy to access the apex of tooth #23.

Neumann flap with intrasulcular incision
This flap offers perfect access for periapical surgery, with sufficient access to the affected bone and lesion-related roots.9Velvart P, Peters CI. Soft tissue management in endodontic surgery.
→ J Endod. 2005 Jan;31(1):4–16. The intrasulcular incision in turn may be triangular or trapezoidal. The most common intrasulcular flap involves a triangular incision with a single vertical releasing incision located distal and one or two teeth distal to the lesion. This flap is characterized by increased tension, the traction forces increasing especially at the fixed extremity (Figs. 10–12). This technique allows easy flap repositioning after periapical surgery.
-

-
Fig. 10
Clinical view before periapical surgery of tooth #21.
-
-
Fig. 11
Detachment of a triangular flap with sulcular incision.
-

-
Fig. 12
Intraoperative view after ostectomy.
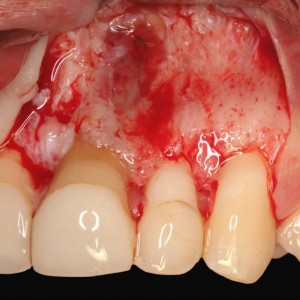
A modification of this flap involves a trapezoidal incision where a horizontal incision is made over the interdental papillae and along the neck of the teeth. Furthermore, two vertical releasing incisions are made on either side of the flap (leaving one or two teeth outside the lesion as a safety margin; Figs. 13–15). The important inconvenience of this technique is that postoperative gingival recession can occur—with a strong esthetic impact in the case of surgery of the anterior maxillary segment.10Von Arx T, Vinzens-Majaniemi T, Bürgin W, Jensen SS. Changes of periodontal parameters following apical surgery: a prospective clinical study of three incision techniques.
→ Int Endod J. 2007 Dec;40(12):959–69.11Von Arx T, Salvi GE, Janner S, Jensen SS. Gingival recession following apical surgery in the esthetic zone: a clinical study with 70 cases.
→ Eur J Esthet Dent. 2009 Spring;4(1):28–45. 12Velvart P, Ebner-Zimmermann U, Ebner JP. Comparison of papilla healing following sulcular full-thickness flap and papilla base flap in endodontic surgery.
→ Int Endod J. 2003 Oct;36(10):653–9.
-

-
Fig. 13
Clinical view before periapical surgery of teeth #12 and 22.

-

-
Fig. 14
Sulcular incision along the gingival margin of the teeth and two vertical releasing incisions distal to the canines.

-

-
Fig. 15
Detachment of the trapezoidal sulcular flap.

Flap with incision at the base of the papillae
This flap was originally described by Velvart13Velvart P. Papilla base incision: a new approach to recession-free healing of the interdental papilla after endodontic surgery.
→ Int Endod J. 2002 May;35(5):453–60. and is characterized by a horizontal incision following the dental sulcus along the neck of the teeth and extending to the base of the papillae. The latter is left adhered for posterior suturing of the flap. A vertical releasing incision is more over made (Figs. 16 & 17). This is a surgically complicated flap requiring adequate surgeon experience. The literature shows this technique to produce less recession at interdental papillary level than a sulcular incision.14Velvart P, Ebner-Zimmermann U, Ebner JP. Comparison of papilla healing following sulcular full-thickness flap and papilla base flap in endodontic surgery.
→ Int Endod J. 2003 Oct;36(10):653–9.
-

-
Fig. 16
Clinical view before periapical surgery of tooth #11.

-

-
Fig. 17
Flap at the base of the interdental papillae to ensure their preservation.

Papilla – preserving incision flap
In this case, a horizontal incision is made following the dental sulcus to the dental papilla, avoiding incision of the latter and tracing the vertical releasing incision at this point.15Kreisler M, Gockel R, Schmidt I, Kühl S, d’Hoedt B. Clinical evaluation of a modified marginal sulcular incision technique in endodontic surgery.
→ Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009 Dec;108(6):e22–8. doi:10.1016/j. tripleo.2009.08.005. This flap is useful in teeth with a generous mesiodistal width, affording an adequate surgical field (Figs. 18–20).
-

-
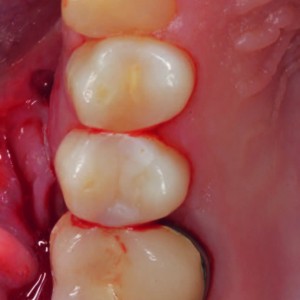
Fig. 18
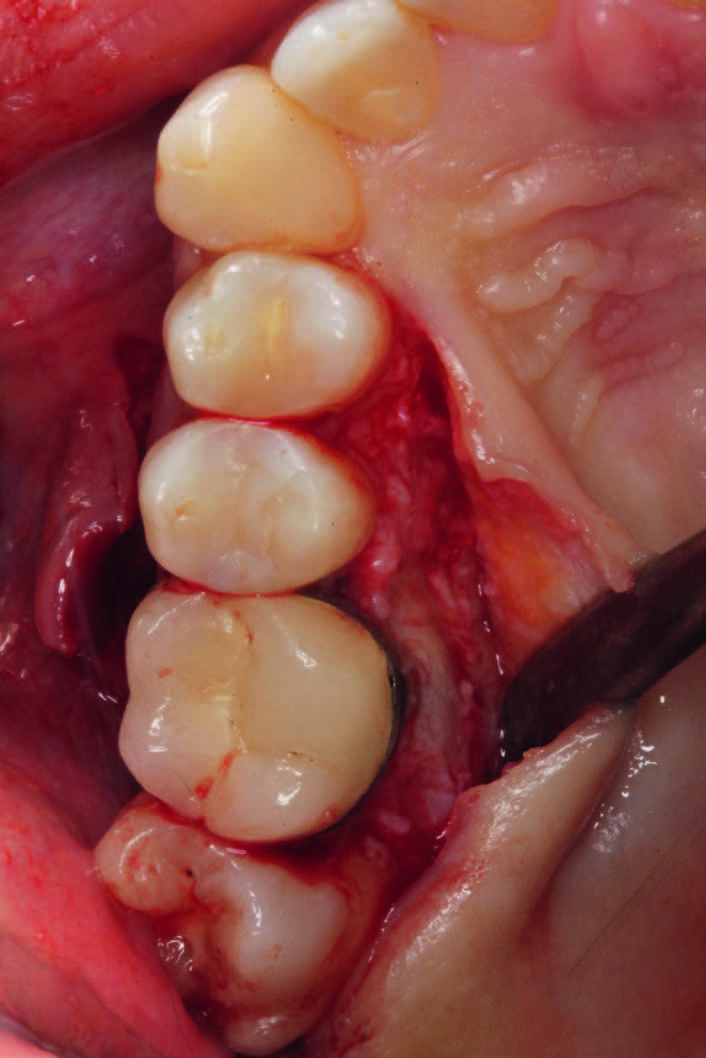
Clinical view before surgery of tooth #34.

-
-
Fig. 19
Design and detachment of a papilla-preserving flap.
-

-
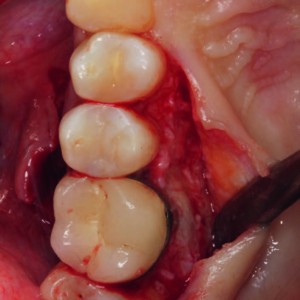
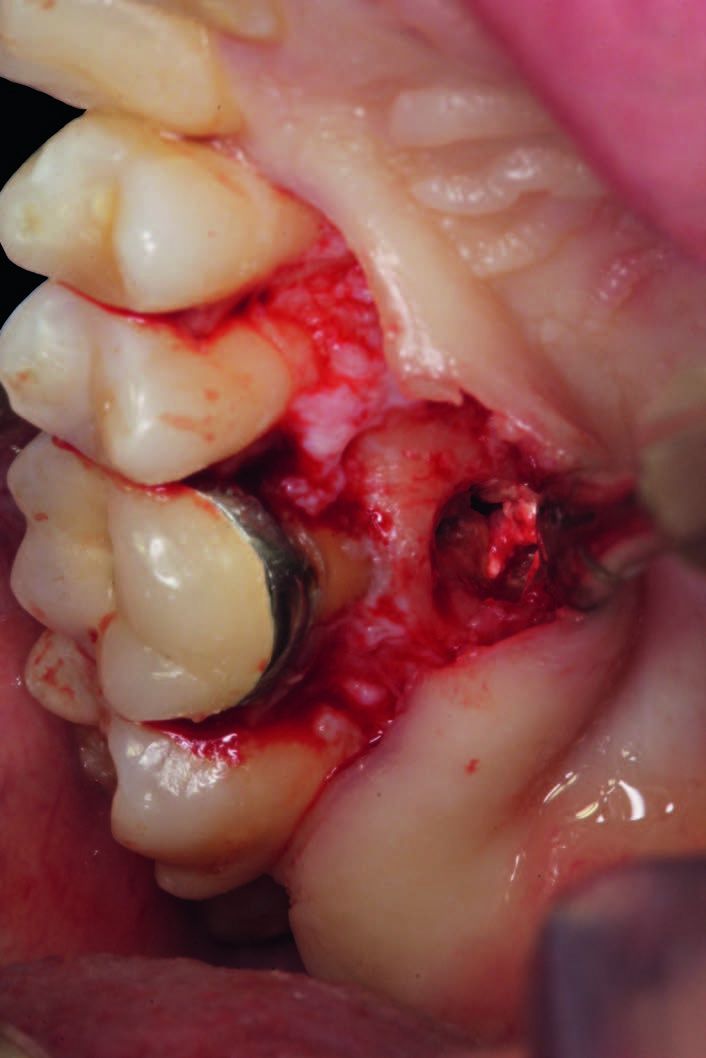
Fig. 20
Intraoperative view after ostectomy.

Palatal flap
A festoon flap is performed at the gingival margins on the palatal side. This flap is used in periapical surgery of the palatal roots of the maxillary molars. If the flap needs to be expanded to gain greater visibility, the incision can be extended mesial to the canine. Palatal releasing incisions are not necessary, though if any such incision is made, it should be performed between the canine and premolar—which represents the vascularization limit between the nasopalatine artery and the anterior palatine artery—or distal to the second molar, behind the emergence point of the anterior palatine artery (Figs. 21–23).16Peñarrocha Oltra D, Cervera Ballester J, Zubeldia Masset P, Luis Calvo Guirado J, Peñarrocha Diago M. Técnica quirúrgica básica.
→ In: Peñarrocha M, Peñarrocha MA, editors. Atlas de cirugía periapical. Madrid: Ergon; 2013. p. 47–97.
-
-
Fig. 21
Clinical view before the festoon palatal flap.

-
-
Fig. 22
Design and detachment of a palatal flap.
-

-
Fig. 23
Ostectomy for accessing the palatal root.
Conclusion
Designing the flap is a key aspect of periapical surgery: It should ensure adequate exposure of the surgical field and allow the surgeon to work quickly and comfortably. Furthermore, there should be no tension capable of complicating the work of the dental professional or of causing patient discomfort, and soft-tissue damage due to retractor compression is to be avoided. A good flap design with delicate manipulation of the soft tissue is necessary for successful periapical surgery.
Competing interests
The authors declare that they have no competing interests.
Interview
with Peñarrocha Diago Maria
Why did you conduct the research reported on in this paper?
For what reasons could others cite your paper?
How could your study’s findings have an impact on dentistry?
What is the relevance of your study’s findings to the daily practice of a dentist?
What are your recommendations for further investigation of the topic of your article?
References
| 1, 2. | ↑ | Arens DE. Flap design. → In: Arens DE, editor. Practical lessons in endodontic surgery. Chicago: Quintessence; 1998. p. 51–64. |
| 3. | ↑ | Vreeland DL, Tidwell E. Flap design for surgical endodontics. → Oral Surg Oral Med Oral Pathol. 1982 Oct;54(4):461–5. |
| 4, 10. | ↑ | Von Arx T, Vinzens-Majaniemi T, Bürgin W, Jensen SS. Changes of periodontal parameters following apical surgery: a prospective clinical study of three incision techniques. → Int Endod J. 2007 Dec;40(12):959–69. |
| 5, 15. | ↑ | Kreisler M, Gockel R, Schmidt I, Kühl S, d’Hoedt B. Clinical evaluation of a modified marginal sulcular incision technique in endodontic surgery. → Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009 Dec;108(6):e22–8. doi:10.1016/j. tripleo.2009.08.005. |
| 6, 11. | ↑ | Von Arx T, Salvi GE, Janner S, Jensen SS. Gingival recession following apical surgery in the esthetic zone: a clinical study with 70 cases. → Eur J Esthet Dent. 2009 Spring;4(1):28–45. |
| 7, 9. | ↑ | Velvart P, Peters CI. Soft tissue management in endodontic surgery. → J Endod. 2005 Jan;31(1):4–16. |
| 8. | ↑ | Peñarrocha M. Técnica quirúrgica. → In: Peñarrocha M, editor. Cirugía periapical. Barcelona: Ars Medica; 2004. p. 45–79. |
| 12, 14. | ↑ | Velvart P, Ebner-Zimmermann U, Ebner JP. Comparison of papilla healing following sulcular full-thickness flap and papilla base flap in endodontic surgery. → Int Endod J. 2003 Oct;36(10):653–9. |
| 13. | ↑ | Velvart P. Papilla base incision: a new approach to recession-free healing of the interdental papilla after endodontic surgery. → Int Endod J. 2002 May;35(5):453–60. |
| 16. | ↑ | Peñarrocha Oltra D, Cervera Ballester J, Zubeldia Masset P, Luis Calvo Guirado J, Peñarrocha Diago M. Técnica quirúrgica básica. → In: Peñarrocha M, Peñarrocha MA, editors. Atlas de cirugía periapical. Madrid: Ergon; 2013. p. 47–97. |



Leave a Reply
Be the First to Comment!